Camrelizumab plus CAPOX (capecitabine plus oxaliplatin) vs. CAPOX alone as initial treatment for gastric or gastro-esophageal junction adenocarcinoma
Peng Z et al, BMJ. 2026;392:e086115
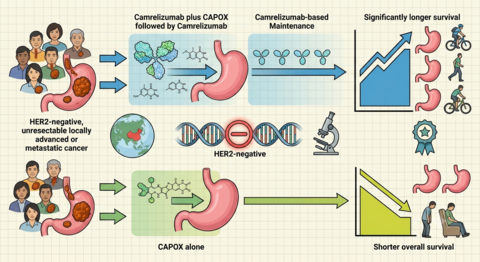
First-line therapy with the PD-1 inhibitor camrelizumab plus CAPOX followed by camrelizumab based maintenance was associated with longer overall survival than CAPOX in HER-2 negative unresectable locally advanced or metastatic cancer in this Chinese phase 3 trial.
Objective: To compare camrelizumab plus capecitabine and oxaliplatin followed by camrelizumab plus apatinib (camre+CAPOX followed by camre+apa), CAPOX alone, and camrelizumab plus CAPOX followed by camrelizumab (camre+CAPOX followed by camre) as initial treatment for gastric or gastro-oesophageal junction adenocarcinoma.
Design: Randomised, open label, phase 3 study.
Setting: 75 hospitals in China, 13 March 2019 to 16 August 2021.
Participants: 885 adults (≥ 18 years) with previously untreated, human epidermal growth factor receptor 2 (HER2) negative, unresectable, locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma. Interventions: Patients were randomised (2:2:1) to receive camre+CAPOX followed by camre+apa, CAPOX only, or camre+CAPOX followed by camre, stratified by Eastern Cooperative Oncology Group performance status, peritoneal metastasis, and programmed death ligand 1 (PD-L1) combined positive score. Assignment to camre+CAPOX followed by camre was introduced midway through enrolment.
Main outcome measures: The primary endpoint was overall survival for camre+CAPOX followed by camre+apa versus CAPOX alone in the PD-L1 positive population (combined positive score > 1) and the overall population who received at least one dose of study drug. Comparisons of camre+CAPOX followed by camre versus CAPOX alone and of camre+CAPOX followed by camre+apa versus camre+CAPOX-camre were descriptive. Safety was assessed in all patients who received at least one dose of study drug.
Results: 352 patients received camre+CAPOX followed by camre+apa, 349 received CAPOX alone, and 177 received camre+CAPOX followed by camre. At the time of data cut off, 454 of 592 (76.7%) deaths had occurred in the PD-L1 positive population and 709 of 878 (80.8%) in the overall population. Overall survival was longer with camre+CAPOX followed by camre+apa than with CAPOX alone in the PD-L1 positive population (median 15.0 vs. 12.5 months; hazard ratio 0.80 (95% CI: 0.65-0.98); one sided p = 0.02) and in the overall population (median 13.5 vs. 12.1 months; hazard ratio 0.80 (0.68-0.94); one sided p = 0.004). Use of camre+CAPOX followed by camre also showed longer overall survival versus CAPOX in the PD-L1 positive population (median 15.3 vs. 12.5 months; hazard ratio 0.76 (0.58-0.97); one sided nominal p = 0.01) and overall population (median 14.2 vs. 12.1 months; hazard ratio 0.80 (0.65-0.98); one sided nominal p = 0.02). No overall survival benefit was observed with camre+CAPOX followed by camre+apa versus camre+CAPOX followed by camre. Treatment related adverse events of grade ≥ 3 occurred in 239 of 352 (67.9%) patients in the camre+CAPOX followed by camre+apa group, 158 of 349 (45.3%) in the CAPOX alone group, and 83 of 177 (46.9%) in the camre+CAPOX followed by camre group.
Conclusions: Initial treatment with camrelizumab plus CAPOX followed by camrelizumab based maintenance was associated with longer overall survival than CAPOX alone in human epidermal growth factor receptor 2 (HER2) negative, unresectable, locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma. Exploratory comparisons between the two camrelizumab based regimens showed no additional survival benefit, with higher rates of treatment related adverse events of grade ≥ 3 and treatment discontinuations when apatinib was added during maintenance.